PARADISE-cohort: hartfalen en COPD samen verhogen de langetermijnmortaliteit, met name HF
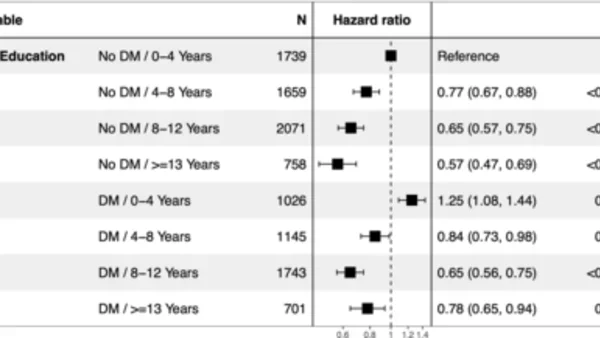
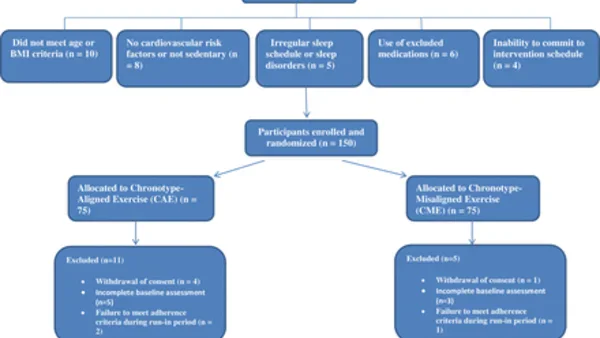
Monocentrische observationele studie (PARADISE-cohort) bij 5.131 patiënten die tussen 2010 en 2019 op de spoedeisende hulp werden opgenomen met acute dyspneu. 3.543 hadden een primaire diagnose hartfalen, 1.588 COPD; in beide groepen had circa 20% het andere ziektebeeld ook. Bij primair HF was concomitante COPD verrassend geassocieerd met lagere ziekenhuissterfte (8,5% vs 11,7%; aOR 0,74), maar wel met iets hogere langetermijnsterfte (aHR 1,22). Bij primair COPD verhoogde concomitant HF de ziekenhuissterfte (7,4% vs 3,4%) niet meer significant na correctie, maar verdrievoudigde wel de langetermijnsterfte (68,7% vs 48,7%; aHR 1,48). Systematische identificatie en optimale behandeling van beide aandoeningen op de SEH zijn cruciaal voor deze hoogrisicogroep.
Abstract (original)
BACKGROUND: Heart failure (HF) and chronic obstructive pulmonary disease (COPD) are leading causes of acute dyspnea in the emergency department (ED) and frequently coexist. However, their combined impact on short- and long-term outcomes in the acute setting remains insufficiently characterized. METHODS: We conducted a monocentric observational study based on the PARADISE cohort, including patients admitted to the ED for acute dyspnea between 2010 and 2019. Patients with a primary diagnosis of HF or COPD were included and stratified according to the presence of the alternate condition. The primary outcomes were in-hospital and post-discharge all-cause mortality, assessed using multivariable regression models. RESULTS: Among 5,131 patients, 3,543 had a primary diagnosis of HF and 1,588 of COPD. Concomitant disease was present in approximately 20% of patients in both groups.In the primary HF cohort, patients with COPD had lower in-hospital mortality compared with those without COPD (8.5% vs. 11.7%, p = 0.014), but similar overall mortality (69.3% vs. 68.9%). After adjustment, COPD remained associated with lower in-hospital mortality (OR 0.74; 95% CI 0.55-0.99; p = 0.050) and with a modest increase in long-term mortality (HR 1.22; 95% CI 1.09-1.36; p < 0.001).In the primary COPD cohort, patients with HF had higher in-hospital mortality (7.4% vs. 3.4%, p = 0.001) and markedly higher long-term mortality (68.7% vs. 48.7%, p < 0.001). After adjustment, HF was not significantly associated with in-hospital mortality (OR 1.54; 95% CI 0.87-2.65; p = 0.13), but remained strongly associated with increased long-term mortality (HR 1.48; 95% CI 1.25-1.76; p < 0.001). CONCLUSIONS: HF and COPD frequently coexist and are both associated with an increased long-term mortality risk, with a greater prognostic impact of HF in patients with COPD. These findings highlight the importance of systematic identification and optimized management of both conditions in this high-risk population.
Dit artikel is een samenvatting van een publicatie in ESC heart failure. Voor het volledige artikel, alle details en referenties verwijzen wij u naar de oorspronkelijke bron.
Lees het volledige artikelDOI: 10.1093/eschf/xvag136
Lid worden van HartVaat.nl?
Gratis — en we stemmen het nieuws en de literatuur af op uw vakgebied.