Polygenic risk independently predicts coronary plaque burden and high-risk plaque in patients with non-obstructive coronary artery disease
- Amsterdam UMC, Amsterdam, Netherlands
- Vascular Medicine, Amsterdam UMC, Amsterdam, Netherlands
- Radiology And Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands
- Cardiology, Amsterdam UMC, Amsterdam, Netherlands
- Amsterdam UMC, Amsterdam, Netherlands
Een polygene risicoscore voorspelt onafhankelijk plaque-belasting en hoogrisicoplaque bij niet-obstructief coronairlijden (Amsterdam UMC).
Bekijk de volledige poster op EAS 2026Poster on board · EAS 2026, Athene
Samenvatting
Achtergrond
Coronairlijden ontstaat door een samenspel van leefstijl en genetische aanleg, maar de huidige cardiovasculaire risicomodellen houden geen rekening met genetisch risico. Een polygene risicoscore (PRS) bundelt miljoenen genetische varianten tot één maat. Of een CAD-PRS samenhangt met plaque-belasting en hoogrisicoplaque (HRP) bij asymptomatisch, niet-obstructief coronairlijden was onbekend.
Methoden
Plaquevolumes werden gekwantificeerd met een AI-gebaseerd kwantitatief CCTA-platform (AI-QCT). Multivariabele regressie (gecorrigeerd voor leeftijd, sekse en risicofactoren) onderzocht de associatie van de PRS met HRP en plaque-belasting. De toegevoegde voorspellende waarde werd vergeleken over drie modellen: SCORE2, SCORE2+PRS, en aanvullend Lp(a) en CRP.
Resultaten
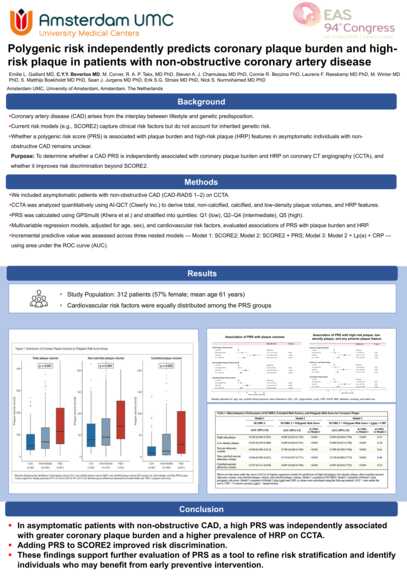
312 patiënten (61 jaar; 57% man). Het mediane totale plaquevolume was meer dan tweemaal hoger in het hoogste dan in het laagste PRS-kwintiel (115 vs 50 mm³; p<0,001). De HRP-prevalentie steeg over de kwintielen van 42% (Q1) naar 69% (Q5; p=0,003). Een hoge PRS (Q5) was onafhankelijk geassocieerd met HRP (OR 3,77; p=0,001) en met 96 mm³ meer totaal plaquevolume. Toevoegen van de PRS aan SCORE2 verbeterde de discriminatie.
Conclusie
Bij asymptomatische patiënten met niet-obstructief coronairlijden voorspelde een hoge PRS onafhankelijk een grotere plaque-belasting en HRP op CCTA, en verbeterde toevoeging aan SCORE2 de risicodiscriminatie. Dit ondersteunt verder onderzoek naar de PRS als hulpmiddel voor risicostratificatie.
Originele Engelstalige samenvatting (zoals ingediend bij EAS 2026)
Background and Aims
Coronary artery disease (CAD) results from the interplay between lifestyle and genetic predisposition. Current cardiovascular risk models do not account for genetic risk. Polygenic risk scores (PRS) aggregate millions of genetic variants into a single metric. Whether a CAD PRS associates with plaque burden and high-risk plaque (HRP) in asymptomatic, non-obstructive CAD remains unknown. We aimed to determine whether a CAD PRS is independently associated with coronary plaque burden and HRP on coronary computed tomography angiography (CCTA).
Methods
Plaque volumes were quantified using an artificial intelligence-based quantitative CCTA (AI- QCT) platform. We used multivariable regression models adjusted for age, sex, and cardiovascular risk factors to evaluate associations of PRS with HRP and plaque burden. Incremental predictive value was assessed across three models: SCORE2 alone (Model 1), SCORE2 plus PRS (Model 2), and Model 2 plus lipoprotein(a) [Lp(a)] and C-reactive protein (CRP) (Model 3), using area under the curve (AUC).
Results
We included 312 patients (age 61 ± 6 years; 57% male). Median total plaque volume was more than twofold higher in Q5 than Q1 (115 vs 50 mm³; p<0.001), with similar gradients for non- calcified (70 vs 39 mm³; p=0.004) and calcified plaque (29 vs 9 mm³; p=0.002). HRP prevalence rose across quintiles: 42% (Q1), 45% (Q2–Q4), and 69% (Q5; p=0.003). High PRS (Q5) was independently associated with HRP (OR 3.77, 95% CI 1.67–8.52; p=0.001) and 96.4 mm³ greater total plaque volume (β=96.4 mm³, 95% CI 52.1–140.6; p<0.001). Adding PRS to SCORE2 improved discrimination for both HRP and percent atheroma volume (Table 1).
Conclusions
In asymptomatic patients with non-obstructive CAD, a high PRS independently predicted greater coronary plaque burden and HRP on CCTA. Adding PRS to SCORE2 improved risk discrimination. These findings support further evaluation of PRS as a tool for risk stratification to identify individuals who may benefit from early preventive intervention.